
Physical HealthTaha tinana
Seeking information about the oesophagus and oesophageal cancer can feel overwhelming or frightening, especially if you’re unsure about what’s ahead for you or a loved one. Having the right information can help lessen some of these feelings. Here you will find reliable information about the oesophagus and oesophageal cancer along with diagnosis, symptoms, risks, treatment, side effects, diet and nutrition and some useful websites to visit.
Nau mai rā, rarau mai rā ki tēnei whārangi mō ngā kōrero e pā ana ki te.
About the oesophagus
Mō te pūkai
The oesophagus, or ‘food pipe’, carries food from the mouth to the stomach. It is about 26 cm long in adults and passes through the chest, behind the windpipe and the heart. The oesophagus has three main sections – the upper, middle, and lower. It carries food and liquids to the stomach using waves of muscle contractions.
Click here to learn more about the oesophagus |
The wall of the oesophagus has several layers (the mucosa, sub-mucosa and muscularis) that help to push food down towards the stomach. Glands in the wall produce mucus to help food slide down more easily when swallowing.
The oesophagus joins to the top part of the stomach (called the cardia) where a valve (the gastro-oesophageal sphincter) keeps the stomach contents from coming back up into the oesophagus.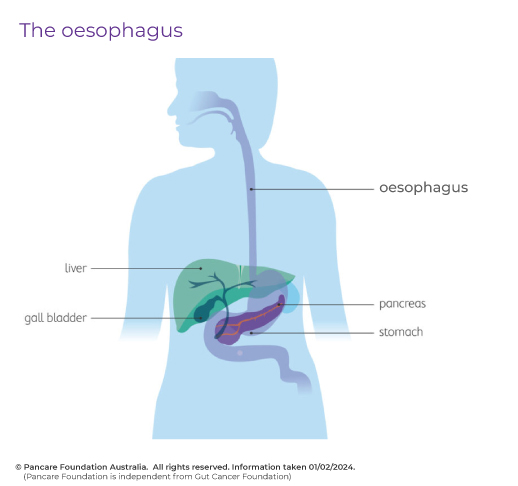

Learn more about the oesophagus and symptoms of the cancer
This video contains sensitive images of organs and the body
What is oesophageal cancer?
Oesophageal cancer occurs when abnormal cells grow out of control. Oesophageal cancer can develop anywhere along the length of the oesophagus, but it most commonly arises in the lower third, towards the stomach end. There are two main types of oesophageal cancer.
Adenocarcinoma
Adenocarcinoma is cancer that begins in the gland cells that produce and release mucus and other fluids most often in the lower part of the oesophagus near the stomach.
Squamous cell carcinoma
Squamous cell carcinoma is cancer that begins in the flat cells lining the oesophagus.
Undifferentiated oesophageal cancer
Sometimes doctors are not able to determine which type of cancer is present because the cells are underdeveloped when looked at under a microscope. These cancers are called undifferentiated cancer.
Symptoms & Risks
Tohumate & Tūraru

Common Symptoms of Oesophageal Cancer
Unexplained symptoms can be worrying for anyone. Here you will find information about some common symptoms of oesophageal cancer and how to manage them. It is important to note that having one or more of these symptoms does not necessarily mean that you have cancer, but if you have new or persistent symptoms that are out of the ordinary for you, it’s really important that you contact your GP to get checked out.
Click here to see common symptoms of oesophageal cancer.
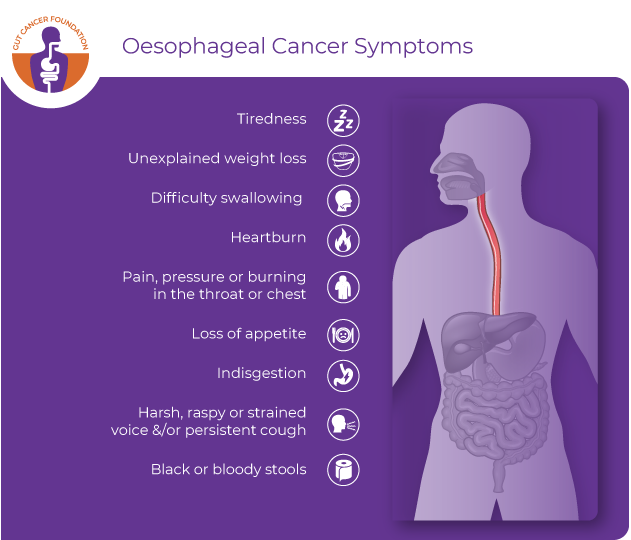
Often there are no early warning signs of oesophageal cancer. If you have any of the below symptoms for more than 2 weeks you should see your GP.
The image below shows what symptoms you might notice if you have oesophageal cancer.
Managing symptoms | Whakahaere i ngā tohumate
You might notice that things change for you physically and emotionally following your diagnosis and you may have even noticed some of these symptoms prior to diagnosis. Understanding them can help you to prepare for them mentally and manage them if they do appear. If you do experience any of these symptoms, let your healthcare team know when you next see them. If they are extreme, or you are worried about them, get in touch with your healthcare team sooner.
Click on the links below to learn about some ways you can manage these changes or symptoms | Pāwhirihia te momo tohumate mō ētahi atu mōhiohio.
Changes in diet | Ngā panonitanga o te whiringa Kai
Many people find that sorting out symptoms related to their diet makes the biggest difference to how they feel. Ask your doctor or nurse for a referral to a dietitian. They can help you with finding food to eat that is gentle on your digestive system.
Nausea | Whakapairuaki
Feeling sick (nauseous) is another common symptom. You may be prescribed anti-sickness medication, or you could try home remedies such as ginger, peppermint, or acupressure bracelets.
Fatigue | Ruha
You are bound to feel tired or exhausted sometimes, so be kind to yourself. Make sure you rest and prioritise what you want or need to do. Give yourself permission to accept offers of help for chores that feel overwhelming. Although you might not feel like it, gentle exercise such as stretching, or a short walk can help combat fatigue.
Intimacy | Mateoha
People of all genders can lose interest in sexual activity during cancer treatment, at least for a time. Although it can feel awkward, talking to your partner about what you find intimate, or soothing can help. There are many ways to be intimate, such as cuddling or gentle touch, or using warmth and comforting language. Your GP may be able to assist with medication or a referral to see a sex and relationship therapist.
Stress, pain, and anxiety | Kohuki, Mamae, Anipā
Simple relaxation techniques can help you cope with stress, pain, and anxiety. Having a warm bath, deep breathing or listening to soothing music are easy things to do at home. You might want to try complementary therapies like reflexology or aromatherapy massage. Talking to others can also help. There are many cancer-specific psychologists available to you in New Zealand – ask your oncologist, nurse, or GP for a referral.
Keep perspective | Kia whakataurite
Each individual will feel and react differently to treatment. What might work for someone else may not always work for you. Acknowledge that not every day will be as easy to manage as the last, and that every day may be different. Focus on what you know works for you and be very gentle with yourself.
Keeping active | Kia kori
Physical activity can also make you feel better, though how much activity will depend on how well you feel. Even a walk round the block or 10 minutes of stretching each day can help.
Risks of developing oesophageal cancer
There are some known risk factors that can increase the chance of oesophageal cancer developing. Having a risk factor does not automatically mean that you will develop oesophageal cancer, but they do increase the likelihood of it happening.
Knowing your risk factors and talking about them with your doctor may help you make more informed lifestyle and health care choices.
Some risk factors are environmental and within your control which is why it is important to understand what they are.
Risks of adenocarcinoma
male gender
obesity
diet low in fresh fruit and vegetables
gastro-oesophageal reflux
barrett’s oesophagus – this should be closely monitored over time to check for any changes
tobacco smoking
alcohol consumption
increasing age.
Risks of squamous cell carcinoma
heavy alcohol consumption
tobacco smoking
increasing age
caustic injury (ingestion of a corrosive substance e.g., acid)
achalasia (a disorder causing difficulty swallowing)
exposure to certain chemical fumes
family history of gastrointestinal disorders such as GORD.
Diagnosis
Tautohunga

Diagnosing oesophageal cancer | Tautohunga mate pukupuku pūkai
Being diagnosed with cancer can be a scary time for anyone. Here you will find information to help you understand some of the terms you might have heard.
In order to diagnose oesophageal cancer, your treatment team will do a range of tests. There might be one test or a mix of tests, some of which are explained below.
Clinical examination | Whakamātau haumanu
If you have symptoms of oesophageal cancer, your doctor may carry out a general clinical examination. The doctor will ask about your medical history to learn about your symptoms and possible risk factors.
Blood Tests | Whakamātau toto
Blood tests are usually taken first to check your blood count and see if your liver and kidneys are working well. Blood tests can also detect tumour markers (chemical substances) that some cancers produce. It is important to note that not all cancers produce these tumour markers, and some other illnesses also produce these markers and so blood tests are often undertaken in combination with other tests.
Upper endoscopy | Tiro oranga whekau runga
During an upper endoscopy, you may be sedated (made sleepy) and then the endoscopist passes an endoscope down your throat and into the oesophagus. The endoscope’s camera is connected to a monitor, which lets the doctor see any abnormal areas in the wall of the oesophagus clearly. Tissue samples can be taken from any abnormal areas. These samples are sent to the lab to check if they contain cancer.
If oesophageal cancer is found and is blocking the oesophagus, certain instruments can be used to help enlarge the opening (dilate) to help food and liquid pass. Upper endoscopy can provide important information about the size and spread of the tumour, which can be used to help determine if the tumour can be removed with surgery.
Barium swallow test and X-ray | Whakamātau horomi waitāmura me te whakaata roto
If you are having trouble swallowing, a barium swallow test may be recommended. You will be asked to swallow a thick chalky fluid called barium which coats the inside lining of the oesophagus and shows any narrowings on X-ray.
Endoscopic ultrasound (EUS) | Oro Ikeike Tiro Oranga Whekau
An endoscopic ultrasound uses a flexible tube with a camera on it (called an ‘endoscope’) which is inserted into the mouth and oesophagus (food pipe). It uses sound waves to create images. Sometimes, there is a small needle on the end that can take fluid or tissue samples (a biopsy) that can be analysed later by the lab.
An EUS can help a doctor see a tumour’s location and size, check whether the cancer has spread to other nearby areas of the body. The images provided by this internal ultrasound have been shown to be helpful in determining whether a tumour can be removed with surgery.
During an upper EUS test, you lie on your left side. A healthcare provider:
gives you an IV sedative to help you relax
sprays your throat with a numbing medicine
places a plastic mouthguard in your mouth. The mouthguard protects your teeth and prevents you from biting down on the endoscope
inserts the ultrasound endoscope through your mouth and into the oesophagus
you shouldn’t feel any pain and you will be able to breathe as usual
when the images and/or biopsy have been taken, the healthcare provider gently removes the endoscope and stops anesthesia. You slowly wake up in a recovery room.
An EUS takes about 1 hour and occurs in an outpatient setting. As you will receive a sedative you will need to take someone with you who can drive you home and stay with you for the remainder of the day.
To prepare for your EUS you may be asked to:
adjust the dosage of your medications such as blood thinners or insulin as recommended by your provider
not eat or drink for a set period of time before the test
take off your clothes on your upper body and change into a hospital gown.
Endoscopic ultrasounds are a very safe procedure, but sometimes minor complications may occur. These include:
sore throat
a small amount of bleeding if a biopsy has been taken
bloating – as air is sometimes pumped through the endoscope during the procedure
small tear in the throat – from insertion of the endoscope
fluid on the lungs – if fluid from your mouth went into the lungs during your procedure
shortness of breath – due to the effects of the sedative.
Computed tomography (CT) scan | Matawaitanga-ā-rorohiko
A computerised tomography scan (CT scan) combines a series of x-ray images that are taken from different angles around the body. You will lie on a motorised bed that passes through a doughnut-shaped tube. It is important that you lay still for good quality images to be taken, and so a strap and/or pillows may be used to help with this. It isn’t painful and usually takes about 1 hour in an outpatient setting.
To prepare for the scan, you may be asked to:
stop eating or drinking for 4 hours before your scan
take off some or all of your clothing and wear a hospital gown for the scan
remove all objects such as jewellery, piercings, dentures, and glasses as they will interfere with the picture quality.
A CT scan uses small amounts of radiation. This is greater than the amount you would get during a simple x-ray, however, it is still a small amount and so the risk to your health is very low. The low dose of radiation you are exposed to during a CT scan has not been shown to cause harm.
Click here for an example of a CT Scan.
Positron emission tomography (PET) | Matawaitanga-ā-rorohiko whakarau pūngao
A PET scan uses a special type of camera that detects radioactive material. A small amount of radioactive material is injected into your arm about 1 hour before the scan which will travel and accumulate in areas of the body where there is higher metabolic activity i.e., where there is disease occurring. The body is then scanned to show where the radioactive material is accumulating.
Allergic reactions can occur due to the radioactive material but are extremely rare.
Similar to the CT scan, you will lie on a motorised bed that passes through a doughnut shaped tube. Sometimes the CT scan and PET scan are combined in the same machine and both types of images are taken at the same time. It is important that you lay still on the bed for good quality images to be taken and so a strap and/or pillows may be used to help with this. It isn’t painful and the whole procedure usually takes about 2 hours in an outpatient setting.
After the procedure you naturally pass the radioactive material out of your body in your urine.
To prepare for the scan you may be asked to | Hei whakarite i mua i te whakaata roto ka pātaihia pea i ēnei pātai:
avoid strenuous exercise for a couple of days before
stop eating 4 hours before your scan.
Click here for an example of a PET scan. *Source: Mediplus.in
PET-CT Scan | Matawaitanga-ā-rorohiko-whakarau pūngao
This scan combines a CT scan with a PET (Positron Emission Tomography) scan. A PET scan uses a small amount of radioactive material, which is injected into your body and is absorbed into your organs and tissues. CT is a type of X-ray.
The combination of the two scans has been proven to be extremely sensitive in detecting small tumours that are undetectable by other imaging procedures or CT alone. PET-CT information can be used to determine what kind of surgery, radiation therapy and chemotherapy is most likely to be successful in managing a patient’s cancer.
Magnetic resonance imaging (MRI) | Whakaahua ponguru autō
An MRI scan uses magnetic fields and radio waves to produce a detailed picture of the body. You will lie on a bed that moves into a tube. It is important that you lay still for good quality images to be taken. It isn’t painful and usually takes between 15 and 90 minutes in an outpatient setting. An MRI scan is very noisy and so you may be given headphones to wear. For those who do not like small spaces it may cause some anxiety. If this is the case, speak to your doctor before your MRI as they may be able to provide you with some relaxation tips or medicine to help you feel calmer.
To prepare for the scan | Hei whakarite i mua i te whakaata roto:
you may be asked to stop eating a few hours before the scan but will be informed beforehand if this is the case
take off some or all of your clothing and wear a hospital gown for the scan
remove all metal objects such as hair clips and piercings and possibly medical patches if you wear one as they may contain metal.
It is important to tell the radiology staff about any metal you have in your body including possible metal fragments in your eye and metal foreign bodies. Objects that have been implanted in your body need to be discussed ahead of the MRI scan as they may cause harm or be damaged. These include pacemakers, aneurysm clips, heart valve replacements, neurostimulators, cochlear implants, magnetic dental implants, and drug infusion pumps.
Click here for an example of an MRI.
It's important to acknowledge that some of these tests can be confronting or sometimes frightening. Taking a friend or whānau member with you can help ease anxiety. Be encouraged to tell staff if you need extra reassurance during the test, you'll find some very compassionate people working in healthcare.
Waiting to have tests carried out | E tāria ana kia whakamātauhia
Even if you have been given an urgent referral for a particular scan or investigation you may have to wait several days or possibly weeks for your appointment. This can be frustrating and worrying, especially if you are already feeling unwell.
Several weeks of testing to confirm a diagnosis or awaiting appointments is relatively common and is unlikely to alter overall outcomes. Cancer growth is considered to be negligible over a period of weeks, and this waiting period is unlikely to cause you harm if your symptoms are stable.
If your symptoms get worse or you start to feel more unwell while you are waiting, it is a good idea to get in touch with your GP or specialist if you already have one. If you cannot get in contact with them, you may need to present to the closest emergency department if your symptoms cannot be controlled at home.
How long will I have to wait for my test results? | Ka hia te roa e tatari ai kia puta ngā kitenga whakamātautau?
Depending on which tests you have had it may take from a few days to a few weeks for the results to come through. Waiting for test results can be an anxious time.
It is a good idea to ask how long you may have to wait when you go for tests. If you think you have been waiting too long, then contact your GP or a specialist to follow up on the progress of your results. Usually, the doctor who does the test will write a report and send it to your specialist. If your GP sent you for the test, the results will be sent to the GP clinic.
You will need an appointment with your specialist or GP to discuss the test results and how they might affect your treatment. Usually, your specialist will discuss your results and plan your subsequent care.
All these tests will give the specialist more information about the cancer such as where it is, if it is growing, and if it has spread. This is called staging. Staging helps to work out the best treatment plan for you.
Oesophageal cancer grade and stage | Te tūātupu me te māhiti o te mate pukupuku pūkai
You may have heard people talk about the stages and grades of cancer. Staging provides an indication of the size of the cancer and if it has spread to other areas of the body. Grading helps your doctor to understand how abnormal the cells look under microscope and how they might behave.
Both staging and grading contribute towards treatment planning.
Grading:
Cancer cells are graded from 1 to 3:
grade 1 (low grade) look most like normal cells. Also known as well differentiated. These cancers are more likely to grow slowly
grade 2 look a bit like normal cells
grade 3 (high grade) look very abnormal and not like normal cells. Also known as undifferentiated. These cancers tend to grow and spread more quickly than low grade cancers.
Staging:
The stage of a cancer tells you how big the cancer is and whether it has spread.
Staging of oesophageal cancer is complicated and depends upon:
what type of oesophageal cancer you have (squamous cell or adenocarcinoma)
the grade of your cancer (how abnormal the cells look)
whether doctors stage your cancer using tests and scans (clinical staging) or after surgery (pathological staging).
There are two ways in which the stage of cancer can be described. One uses numbers (stage 1, 2 etc) and the other uses letters and numbers (T1, N0, M0 etc) also known as TNM (Tumour-Nodes-Metastases) staging. The cancer may be described in one or both ways by your healthcare team.
Click here to learn more about the stages of cancer | Pāwhirihia ki kōnei mō ngā kōrero āpiti
TNM (Tumour-Nodes-Metastases) staging
TNM staging is the most common type of staging for oesophageal cancer. The TNM gives a number according to tumour size (T), how many lymph nodes are affected (N), and how far the cancer has spread, or metastasised, to distant parts of the body (M). This may be expressed as, for example, T1, N0, M0. This information is used to help decide the best treatment.
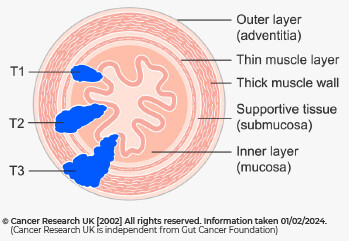
T1 | The cancer has grown no further than the layer of supportive tissue (submucosa). It's split into 2 further stages:
|
T2 | The cancer has grown into the muscle layer of the wall of the oesophagus. |
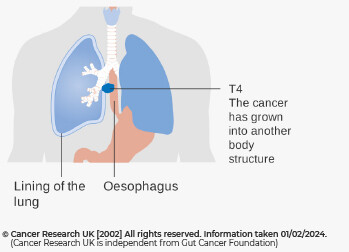
T3 | The tumour has grown into the membrane covering the outside of the oesophagus (adventitia). |
T4 | The tumour has grown into other organs or body structures next to the food pipe. Its divided into 2 further stages:
|
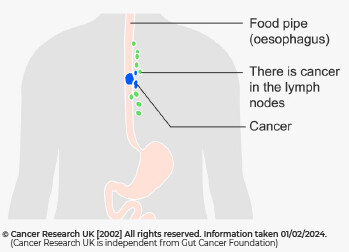
N0 | There are no lymph nodes containing cancer cells. |
N1 | There are cancer cells in 1 or 2 nearby lymph nodes. |
N2 | There are cancer cells in 3 to 6 nearby lymph nodes. |
N3 | There are cancer cells in 7 or more nearby lymph nodes. |
M0 | The cancer has not spread to other organs. |
M1 | The cancer has spread to other parts of the body. |
Stages using numbers
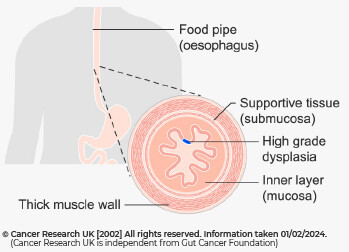
Stage 0 | Also known as high grade dysplasia or carcinoma in-situ, stage 0 means that there are severely abnormal cells in the inner lining of the oesophagus. It is only in the top layer of cells lining the inside of the oesophagus (the epithelium). It has not started to grow into the deeper layers. |
Stage 1 | The cancer is growing into the oesophagus lining but usually hasn’t spread beyond the thick muscle of the oesophagus wall and hasn’t spread to nearby lymph nodes. Some people with squamous cell cancer may have cancer in 1 or 2 nearby lymph nodes. It has not spread to other body parts. | |
Stage 2 | The cancer may have spread to the outer layer of the oesophagus and also may have spread into 1 or 2 nearby lymph nodes. The cancer has not spread to other parts of the body. | |
Stage 3 | The cancer may have spread outside of the oesophagus into nearby tissue and may have spread to up to 6 nearby lymph nodes. It has not spread to any distant body parts. | |
Stage 4 | Also called Advanced Cancer. There are sub-stages of stage 4 cancer. Stage 4a
Stage 4b
|
Prognosis (Life expectancy) | Matapaenga (Te wā ora)
Like any cancer there are many things that can impact on survival rates, so it is best to talk to your cancer specialist for guidance about your own care and outcomes. Remember, even with a diagnosis, no one can know for certain how long anyone will live. Estimates of life expectancy are based on historical data, however treatments are becoming more effective over time which changes these estimates.
Prognosis is usually improved the earlier the cancer is detected. Your doctor will be able to give you the best idea of prognosis.
Often, statistics talk about survival rates which are taken from an average of other patients. These are usually described in 1, 5 and 10-year survival rates. A 10-year survival rate is the proportion (or percent) of people who have not died 10 years after having cancer, however many people live much longer than this.
Click here to view oesophageal cancer statistics related to morbidity (number of diagnoses) and mortality (survival rate).Remember that everyone is different, and statistics are only a guide.
There are around 375 new diagnoses of oesophageal cancer each year in New Zealand.
Oesophageal cancer is more common in men than in women. It usually occurs in people over the age of 60, although can occur at a younger age.
Men are twice as likely to be diagnosed with cancer of the oesophagus than women, and Māori experience both higher rates of incidence and approximately 40% higher mortality that non-Māori.
Overall, the survival rate remains low at 36% at year one, 12.5% at year 5, and 10.4% at year 10. Around 251 New Zealanders die from oesophageal cancer each year.
We know that these rates increase the earlier the cancer is found and can be as high as 47% if the tumour is discovered at an early stage.
Remember that everyone is different, and statistics are only a guide.
Seeking a second opinion | E rapu ana i te whakaaro kē atu
Following diagnosis, some people choose to request a second opinion because they want to have peace of mind that they have explored all options and opinions available to them before starting treatment.
If you would like to know more about your care team and how to seek a second opinion, click this link.
Treatment
Ngā momo rongoā

Treatment options | Ngā kōwhiringa rongoā
There are a number of treatment options available, and it may feel confusing and unsettling not knowing which will be the best for you.
Treatment of oesophageal cancer depends on its location, the stage of the cancer (how advanced it is at the time of diagnosis), and whether the person is otherwise medically fit.
The choice of treatments will be discussed with you and your whānau and your preferences will be considered. Your treatment will be discussed by a multidisciplinary team (MDT), which means that experts in different areas of cancer treatment (e.g., surgeons, gastroenterologists, pathologists, radiologists, oncologists, and nurses) come together to share their expertise in order to provide the best patient care.
It is also important to note that more than one treatment may be needed to get the best results.
The prognosis after treatment depends on the stage and the treatment given. In the best circumstances, cure is possible. If cure is not possible, the symptoms caused by the cancer can often be alleviated.
See below to read more about the treatment options | Tirohia atu ētahi kōwhiringa rongoā ki raro nei
*Not all the options below will be applicable to everyone's situation. Some treatments listed may not be funded and would require the patient to pay directly. It is important to discuss all your options with your specialist team.
Surgery | Poka tinana
Surgery is the most common curative treatment for oesophageal cancer. There are a number of different surgical options available depending on the size and location of the cancer.
Open radical oesophagectomy:
The cancerous portions of the oesophagus, top portion of the stomach and neighbouring lymph nodes are removed.
Click here to view a diagram of the surgery | Pāwhirihia ki kōnei kia tirohia ngā hoahoa o te poka tinana
Minimally invasive oesophagectomy:
Keyhole operation to achieve similar results to the standard open radical approach.
Endoscopic mucosal resection (EMR):
Endomucosal resection can be an option for very early tumours, particularly in patients unlikely to tolerate major surgery.
EMR is where a thin flexible tube (endoscope) with a tiny camera and light on the end is passed through the mouth and into the oesophagus (food pipe). Instruments are passed down through the pipe to the area where the cancer is. A small amount of fluid is injected under the cancerous cells to make them stand out from the rest of the healthy tissue. The cancerous cells are then removed.
Learn more about EMR
Endoscopic mucosal resection usually occurs in the endoscopic department of the hospital. You will be given a sedative to make you sleepy or sometimes a general anaesthetic so you will be fully asleep. The procedure usually takes 30-90 minutes, and you will not remember the procedure when you wake up.
Whether you are able to go home the same day or have to stay overnight in hospital will depend on your own treatment circumstances. You will need someone to drive you home and stay with you for the rest of the day. You will usually only be allowed to drink fluids for the first couple of days following the procedure.
Some common symptoms may include:
mild chest pain like heartburn
mild discomfort when you eat food
bloating and discomfort lasting a few hours.
Risks are a part of any procedure. Your doctor will have weighed up the potential risks and benefits. Below are some possible risks of the procedure:
bleeding – contact the hospital if you start bleeding from your mouth or if your faeces (poo) is black
a sore throat that can last for up to 24 hours – contact the hospital if you have severe pain in your throat, chest, or tummy (abdomen)
fluid going into your lungs from your mouth – this rarely happens as a nurse removes the fluid from your mouth during the procedure
a reaction to the sedative making you breathless
a small tear in the lining of your oesophagus or stomach – this is rare, treatment is antibiotics and fluids through a drip or surgery to repair the tear
narrowing of the oesophagus that develops a while after the procedure – if it happens you have another endoscopy to stretch the oesophagus.
Click here to view a diagram of the surgery.
Radiation therapy | Haumanu iraruke
Radiation therapy may be used in conjunction with surgery and/or chemotherapy. Radiation therapy uses x-rays to kill cancer cells and stop the cancer growing.
Radiotherapy uses ionising radiation to damage the deoxyribose nucleic acid (DNA) of cancerous cells, causing them to die.
Radiotherapy is commonly used in the treatment of oesophageal cancer in a palliative setting to assist with symptom control.
Radiotherapy can be given to treat symptoms related to cancer that are causing problems. These can happen because the growth of the tumour narrows the gullet, causing swallowing difficulties, or it can cause pain or bleeding. Radiotherapy can relieve this pressure by shrinking the tumour.
External beam radiation therapy | Haumanu Iraruke pūhihi rāwaho
Getting radiation therapy is similar to getting an X-Ray but the radiation is stronger. It is a painless procedure which involves lying on a table and a large machine rotating around you. It is directed at the tumour to try to kill the tumour or stop the cancer cells growing without damaging the healthy tissue nearby. Radiotherapy is usually performed in an outpatient clinic. It usually takes place everyday Monday to Friday and lasts for about 10-20 minutes. Your treatment team will be able to tell you how many weeks you will need radiotherapy for.
Click here for an example of external beam radiation therapy | Pāwhirihia ki kōnei kia tirohia te hoahoa Haumanu Iraruke pūhihi rāwaho
Chemotherapy | Haumanu matū
Chemotherapy uses drugs to kill cancer cells and stop the cancer growing and dividing.
Chemotherapy is a drug which is administered either by swallowing tablets; through an injection; or through infusion which is a small tube that is inserted into a vein. The drug works by moving through the blood stream to kill the cancer cells. Unfortunately, some healthy cells can also be harmed leading to side effects. Chemotherapy can be given alone or in combination with other therapies such as targeted therapy, surgery, or radiation. It is usually administered in an outpatient clinic and sometimes a hospital stay is needed if the doctor wants to monitor you following treatment.
Click here for an example of chemotherapy infusion | Pāwhirihia ki kōnei kia tirohia te hoahoa whāuru haumanu matū
Chemoradiation | Hauhau iraruke
Sometimes patients will begin treatment for oesophageal cancer with radiation therapy along with chemotherapy. This combination treatment is called chemoradiation. Patients undergoing curative treatment will have chemoradiotherapy followed by surgery. Having chemotherapy and radiotherapy together can make the side effects of treatment worse. It may not be suitable for people who have other health problems. Your cancer doctor or specialist nurse can give you more information about chemoradiation and its possible side effects.
Photodynamic therapy | Haumanu whakaahua taineke
Photodynamic therapy is where laser-sensitive chemicals are injected into the tumor site. A laser beam then targets the chemicals to destroy the tumor. This therapy is more commonly utilised for treatment of pre-cancers in high risk regions or when surgery is not possible for palliative purposes. This treatment is not common in New Zealand.
Radio Frequency Ablation | Tūnguru iarere
Radio frequency ablation utilises a radio frequency generator via a probe (device). The energy is transmitted to the target tissue causing it to heat up. The heat destroys the target tissue and the body replenishes it with normal cells. This is sometimes used to manage Barret's oesophagus but is not a common treatment for cancer.
Argon Plasma | Wētoto hauhauhā
Argon plasma therapy involves direct thermal injury to precancerous cells. The body then recovers and replenishes the area of injury with normal cells. This is sometimes used to manage Barret's oesophagus but is not a common treatment for cancer.
Stenting | Whakauru ngongo roa
If a tumour is blocking the oesophagus, it can become hard to swallow. This is called dysphagia. In order to make it easier for you to swallow, your doctor may recommended that you have an oesophageal stent. The stent is a hollow tube that is placed in your oesophagus in the area of the tumour to hold the area open. The stent expands to allow fluid and food to pass into the stomach more easily.
On the day of the procedure your doctor will use an endoscope to look into your oesophagus. An endoscope is a flexible tube with a camera that goes through your mouth into your oesophagus. The doctor will place the stent with a fluoroscopy (a real-time X-ray). After the stent is in the right position, you will be allowed to go home. It is important to follow the instructions given to you when you leave hospital about slowly introducing food. The stent does not treat the cancer but will allow you to eat and drink easier.
Clinical trials | Whakamātau haumanu
You may be eligible to take part in a clinical trial, which is a type of research study that investigates new or specialised therapies or treatments. While you are discussing therapy options with your care team, it is a good idea to ask about clinical trials that may be suitable for your condition and discuss whether participating may be right for you.
Being involved in a clinical trial may be beneficial in that you may access the latest treatments before they become generally available. Additionally, clinical trial participation is often associated with closer monitoring of your care and condition and potentially improved outcomes.
Palliative care | Pairuri
A specialist may refer a patient to palliative care services, but this doesn’t always mean end-of-life care. Today people can be referred to these services much earlier if they’re living with cancer. Palliative care can help one to live as well as possible including managing pain and symptoms. This care may be at home, in a hospital or at another location one prefers. Additional supportive care (treatment or services that support you through a cancer experience) are also available.
Traditional Māori Healing | Rongoā Māori
Rongoā Māori is a body of knowledge that takes a holistic view to wellbeing and treatment. In particular, it focuses on hinengaro (mind), wairua (soul), mauri (life essence), ngā atua (Gods) and te taiao (the environment).
There are many providers who are able to provide rongoā services. Your Māori Health team at the hospital will be able to connect you with one nearest to where you live.
See the below websites for more information on rongoā Māori
Other complementary therapies
Complementary therapies are treatments that are used alongside standard treatments. They are often used to boost the immune system, relieve symptoms, and enhance the effectiveness of standard treatments.
Speak to your doctor if you intend to use complementary therapies to ensure that they will work well alongside your treatment.
Some examples of complementary therapies are:
acupuncture
meditation and mindfulness
music therapy
massage
aromatherapy
naturopathy
tai chi
pilates
visualisation or Guided Imagery
spirituality.
Click here to find out more about complementary therapies.
Side Effects from Treatment
Ngā mate āpiti

Side effects of oesophageal cancer treatment | Ngā mate āpiti o te maimoatanga mate pukupuku pūkai
As with any medical treatment, you may experience side effects from your cancer treatment. This is perfectly normal and can be a sign that the treatment is working, although it may feel unpleasant. Side effects vary from person to person and depend on the type of treatment, the part of the body treated, and the length and dose of treatment. Most side effects are temporary and go away after treatment ends. Below you can find information on some common side effects of treatments and how you can manage them to improve your daily well-being.
You may experience side effects other than those discussed here.
If you experience side effects, let your healthcare team know when you next see them. If the symptoms feel extreme or are worrying you, get in contact with your oncology team sooner.
Common side effects of oesophageal cancer treatments | Ngā mate āpiti tōkau o ngā maimoatanga mate pukupuku pūkai
Click on each treatment to learn more about the side effects of that treatment | Pāwhirihia i ia momo rongoā kia tirohia i ngā mate āpiti e hāngai ana
Surgery | Poka tinana
Some side effects of surgery are due to the anaesthesia and should fade shortly after the surgery. These include:
nausea | whakapairuaki
vomiting | whakaruaki
dizziness | takaānini
agitation | pōkeka.
Other side effects are due to the surgical procedure itself which should subside shortly after surgery. These include:
fatigue | ruha
pain at the site of the surgery | mamae wāhi poka.
Some additional side effects may present due to the disruption to your digestive system as a result of the surgery and could take weeks or months to recover from. These include:
diarrhoea and malabsorption | kotere me whākapi miti
weight loss | heke taumaha
loss of appetite | minangaro
feeling full quickly | pūnaunau wawe.
Chemotherapy and biological therapies | Haumanu matū, koiora
Chemotherapy treatment kills cancer cells, but in the process, damages normal healthy cells which causes side effects. These side effects vary from person to person and depend on the type of treatment, the part of the body treated, and the length and dose of treatment. Below are some common side effects of this.
nausea and vomiting | whakapairuaki & whakaruaki
loss of appetite | minangaro
feeling full quickly | pūnaunau wawe
diarrhoea and constipation | kotere me te kōroke
fatigue | ruha
weight loss | heke taumaha
sore mouth or throat | mamae o te waha/ korokoro
taste changes | panonitana rongo tawara
hair loss | whakahewa
dry or itchy skin | kiri mangeo
foggy brain.
Some chemotherapy side effects can be life threatening therefore it is important to go to contact your oncology team or go to your nearest emergency department immediately if you experience any of the following and let them know that you are undergoing chemotherapy treatment. These include:
fever or chills
pain in your chest or difficulty breathing
severe diarrhoea
vomiting that is not eased with anti-sickness medication
bleeding from the gums or nose that doesn’t stop
pain or blood present when passing urine.
Radiation therapy | Haumanu iraruke
Radiation therapy is used to kill cancer cells, but it can also kill some healthy cells near to the cancer site too. Although radiation therapy itself does not hurt, you may experience some symptoms afterwards due to the affect the radiation has on the healthy cells. These symptoms may include:
nausea and vomiting | whakapairuaki & ruaki
loss of appetite | minangaro
feeling full quickly | pūnaunau wawe
diarrhoea and constipation | kotere & kōreke
fatigue | ruha
similar to a sunburn - at the radiation site | mamae tīkākā
weight loss | heke taumaha.
Managing symptoms and side effects | Whakahaere tohumate me ngā mate āpiti
Click on the symptoms below to find information on how to manage symptoms and side effects | Pāwhirihia i ia momo tohumate mō ngā mōhiohio kia whakahaere ai ngā tohumate me ngā mate āpiti
Fatigue | Ruha
A common side effect of treatment is feeling constant tiredness (fatigue). Treatment or the cancer itself can reduce the number of red blood cells in your body, resulting in anaemia, which can make you feel very tired.
Tips to manage fatigue | Ngā kupu āwhina mō te whakahaere i te ruha:
Use your energy wisely
plan ahead for when you feel too tired to cook
shop online for groceries
bulk cook meals you can store in the freezer
cook when you have more energy
ask and accept offers of help with shopping and cooking from whānau and friends
use home delivery services such as Meals on Wheels or other companies that bring pre-prepared food to you. You can ask for help to access these via your social worker
keep snacks handy in your bag or car.
Activity can help with fatigue
regular, gentle exercise can help improve fatigue and your appetite
activity can mean many things – walking, stretching, even vacuuming!
set small goals. Set a timer for five minutes and see what you can manage in this time
eat with others.
Loss of appetite | Kore hiakai
It can be discouraging to lose your appetite. You may lose your appetite because of the effects of cancer itself, the treatment, or other side effects, such as feeling sick, not enjoying the smell of food, or feeling upset. To help you can:
eat small amounts often, e.g., every 2–3 hours. Keeping to a regular eating pattern rather than waiting until you are hungry will mean your body gets the nourishment it needs to
use a smaller plate – a big plate of food may put you off
eat what you feel like when you feel like it. Have cereal for dinner or a main meal at lunch
include a variety of foods in your diet
sip fluids throughout the day
replace water, tea and coffee with drinks or soups that add energy (kilojoules/calories), such as milk, milkshake, smoothies, replacement drinks or soup
relax dietary restrictions – maintaining your weight or regaining weight you have lost is more important than avoiding full-fat and other high-energy foods
gentle physical activity can stimulate appetite – take a short walk around the block
eat with others
keep snacks handy e.g., in your bag or car so you can eat on the go
talk to your dietitian about liquid meal replacements that might be easier to digest.
Taste or smell changes | Rongo kakara me te hā
Some treatments such as chemotherapy can change the way food and/or drink taste or smell. It may taste bland or metallic.
Tips on managing changes in taste include:
add extra flavour to food if it tastes bland – like fresh herbs, lemon, lime, ginger, garlic, soy sauce, honey, chilli, or pepper
experiment with different food, as your tastes may change
if meat tastes bad during treatment, replace it with other protein sources like cheese, eggs, nuts, dairy foods, baked beans, lentils, or chickpeas
add small amounts of sugar to food if it tastes bitter or salty
use a straw when drinking
change from using metal cutlery to plastic or bamboo cutlery.
Tips on managing changes in smell include | Ngā kupu āwhina mō te whakahaere i ngā panoni rongo kakara:
eat cold food or food at room temperature (hot food smells more)
reheat pre-prepared meals in the microwave so the cooking smell doesn’t put you off
stay out of the kitchen, if possible, when food is being prepared
ask family or friends to cook
use the exhaust fan, open the kitchen window, or cook outside to help reduce cooking smells.
Nausea and vomiting | Whakapairuaki me te ruaki
Feeling sick and vomiting are often side effects of cancer, its treatment, or some medicines. They often occur together, but not always.
Nausea | Whakapairuaki
Nausea is stomach discomfort and the sensation of wanting to vomit. Nausea can be a precursor to vomiting the contents of the stomach and may be caused by treatment, stress, food odours, gas in the gastrointestinal tract, motion sickness or even the thought of having treatment.
Tips on how to cope with nausea | Ngā kupu āwhina ki te morimori i te whakapairuaki:
have a light snack before treatment and wait a few hours before eating again
eat small meals 5–6 times during the day. Going without food for long periods can make nausea worse
snack on dry or bland foods, e.g., crackers, toast, dry cereals, bread sticks or pretzels
choose cold foods or foods at room temperature instead of hot, fried, greasy, or spicy foods
eat and drink slowly and chew your food well
try foods with ginger, e.g., ginger biscuits, or ginger beer
avoid foods that are overly sweet, fatty, fried, spicy, or oily, or that have strong smells
brush teeth regularly to help reduce unpleasant tastes that may make you feel nauseated
do not eat your favourite food when feeling nauseated to avoid developing a permanent dislike
suck on hard lollies – flavoured with ginger, peppermint, or lemon
try ginger food and drink items, such as candied ginger, ginger beer, ginger ale, or ginger tea. Talk to your dietitian doctor or pharmacist about ginger supplements
take anti-nausea medicines as prescribed. Let the doctor know if the medicines don’t seem to be working.
Vomiting | Ruaki
Vomiting is the forcible emptying (“throwing up”) of stomach contents through the mouth. Vomiting can follow nausea and may be caused by treatment, stress, food odours, gas in the gastrointestinal tract, motion sickness or even the thought of having treatment.
Vomiting is more serious than nausea. Vomiting can cause dehydration and increase the risk of malnutrition. See a doctor if you are vomiting for more than one day, especially if you cannot keep water down as you may become dehydrated.
Tips on how to cope with vomiting | Ngā kupu āwhina ki te morimori i te ruaki:
take small sips of water or clear liquids, such as ginger ale, soda water or sports drinks like Gatorade or Hydrolyte. Dilute sweet drinks. If you feel like a fizzy drink, open it, and let it sit for 10 minutes or so, and drink it when it’s a bit flat
sucking on crushed ice cubes or an ice block can be soothing
once you can keep clear liquids down try some different drinks, such as consommé and clear broths, weak tea, herbal tea, fruit drinks, beef, and chicken stocks
have small, frequent meals and snacks throughout the day
introduce bland, starchy foods, such as plain biscuits, bread or toast with honey or jam, peanut butter, rice, yoghurt, or fruit. Attempt small, frequent servings at first
consume a little bit more each time until you are eating a well-balanced diet.
Chewing and swallowing | Ngaungau me te horomi
After treatment chewing and swallowing may be difficult and painful. Surgery, radiotherapy, and chemotherapy can cause temporary problems. People with dentures who have lost weight may also find their teeth become loose, which can make eating difficult.
Signs that you are having problems with chewing and swallowing include taking longer to chew and swallow, coughing or choking while eating or drinking, or food sticking in your mouth or throat like a ball.
Tips on chewing and swallowing | Ngā kupu āwhina mō te ngaungau me te horomi:
change how you prepare your food by chopping food up into smaller pieces or pureeing
let your doctor know that you are having issues and get a referral to see a speech pathologist and dietitian
a speech pathologist can monitor your ability to swallow and suggest modifications to the texture of your food once your ability to swallow and chew begins to improve. A dietitian can ensure you are meeting your nutritional needs.
Mouth changes | Ngā panonitanga o te waha
Some chemotherapy drugs and some pain medicines can make your mouth dry, cause mouth ulcers, or change the amount of saliva in your mouth. A dry mouth can increase the risk of tooth decay and infections such as oral thrush, which will make eating harder.
Ulcers may also be present in your digestive tract, causing discomfort in the stomach or bowel and diarrhoea.
Tips to lessen discomfort with mouth sores | Ngā kupu āwhina ki te whakamauru i ngā harehare waha:
suck on ice cubes
eat soft foods – stews, soups, scrambled eggs, and smoothies
cold foods and fluids may be more comfortable than hot ones
avoid ‘coarse’ foods that can irritate your mouth, such as crackers, toast, nuts, and seeds
avoid spicy or very hot foods
use a straw and direct liquids away from the areas where mouth sores are most painful
talk to your doctor about medication or mouth washes to help manage the pain and allow you to eat more comfortably.
Tips to relieve a dry mouth | Ngā kupu āwhina ki te whakamauru i te waha maroke:
suck on ice cubes
keep your mouth clean with regular mouthwashes to prevent infections
gargle with 1⁄2 tsp salt or 1 tsp bicarbonate of soda in a glass of water
choose an alcohol-free mouthwash to avoid irritating your mouth further
use a soft toothbrush when cleaning your teeth
ask your dentist or health care team about suitable mouth rinses or oral lubricants
limit alcohol and coffee as these are dehydrating fluids and avoid smoking
avoid ‘coarse’ foods that can irritate your mouth, such as crackers, toast, nuts, and seeds
avoid spicy or very hot foods
soften food by dipping it into milk, soup, tea, or coffee
moisten with sauce, gravy, cream, custard
sip fluids with meals and throughout the day
chew sugar-free gum to stimulate the flow of saliva.
Changes in bowels- constipation and diarrhoea | Ngā panonitanga o ngā kōpiro
Living with cancer and its treatments can result in changes to your bowel habits. This could be differences in the appearance, consistency, and/or the smell of your stools.
Constipation | Kōroke
This is when your bowel motions are infrequent and difficult to pass. It can be caused by different factors including regularly taking opioid medicines; having a diet low in fibre; not getting enough exercise; not having enough fluids to drink (dehydration); or having a low overall food intake.
Tips on how to manage constipation | Ngā kupu āwhina mō te whakahaere kōroke:
soften stools by drinking 8–10 glasses of fluid a day, e.g., water, herbal tea, milk-based drinks, soup, prune juice
eat foods high in fibre, e.g., wholegrain breads, cereals, or pasta; raw and unpeeled fruits and vegetables; nuts and seeds; legumes and pulses
if you are increasing the amount of fibre in your diet, increase fluids to prevent the extra fibre making constipation worse
ask your doctor about using a laxative, stool softener and/or fibre supplement
exercise – check with your doctor, exercise physiologist or physiotherapist about the amount and type of exercise that is right for you.
Diarrhea | Kotere
This means your bowel motions are watery, urgent, and frequent. You may also get abdominal cramping, wind, and pain. Frequent loose stools can occur because you are not digesting food or absorbing nutrients properly. Cancer treatment, medicines, infections, reactions to certain foods and anxiety can all cause diarrhea.
Diarrhea can result in dehydration, so it’s important to stay hydrated by drinking extra fluids. Every time you have a loose bowel movement you should drink an extra cup of non-caffeinated fluid. If you have diarrhea for several days, see your doctor so they can determine the cause and help to manage your diarrhea. Your doctor may decide to prescribe you anti-diarrhea or over-the-counter medication.
Tips on how to manage diarrhea | Ngā kupu āwhina mō te whakahaere kōtere:
drink plenty of fluids to avoid becoming dehydrated. Water and diluted cordials are better than high-sugar drinks, alcohol, or caffeinated fluids – remember signs of dehydration are smaller amounts of dark urine
choose low-fibre foods, e.g., bananas, mashed potato, rice, pasta, white bread, oats, steamed chicken without the skin, white fish
avoid foods that increase bowel activity, e.g., spicy, fatty, or oily foods, caffeine, alcohol, or artificial sweeteners
try soy milk or lactose-free milk if you develop a temporary intolerance to milk (lactose)
don’t eat too many raw fruit and vegetable skins and wholegrain cereals as they may make diarrhea worse
avoid foods and drinks that are high in sugar, such as cordial, soft drinks and lollies
avoid foods sweetened with artificial sweeteners such as sorbitol, mannitol, and xylitol. These are often marketed as ‘sugar-free’
it may also help to eat small, frequent meals throughout the day, rather than three large meals.
Heartburn (Indigestion) | Tokopā
Some cancers and treatments can cause heartburn, which is a burning sensation in the upper chest, oesophagus and/or throat. It is caused by the contents of the stomach coming back up into the oesophagus (reflux).
Heartburn may make you feel too uncomfortable to eat much, which could lead to weight loss. If the tips below do not relieve heartburn, let your doctor know as medication may help to prevent or manage these side effects.
Tips to manage heartburn | Ngā kupu āwhina mō te whakahaere tokopā:
avoid large meals; try to eat 3 small meals and 3 small snacks throughout the day
eat slowly and take the time to enjoy your meal
avoid wearing tight clothing while eating, especially belts
sip fluids between meals, rather than drinking large amounts at mealtimes
limit or avoid foods that may make heartburn worse, e.g., chocolate, highly seasoned spicy foods, high-fat foods (e.g., fried food, pastries, cream, butter, and oils), tomato and tomato products, citrus fruits, coffee (including decaf), strong tea, soft drinks, and alcohol
straight after eating, sit upright for at least 30 minutes and avoid lying down or activities that involve bending over (e.g., gardening).
Peripheral neuropathy | Pūtau Iotaiaki mōwaho
Peripheral neuropathy is caused by damage to the peripheral nerves. These are the nerves in the body outside the brain or spinal cord. Peripheral neuropathy may be caused by cancer, cancer treatments or other health problems. It most commonly affects the hands and feet. Peripheral neuropathy caused by cancer treatment will get better over time with proper treatment and care.
The most common symptoms of peripheral neuropathy can include | Ngā kōrero tōkau mō te Pūtau Iotaiaki Mōwaho:
tingling, burning, numbness or pain in the hands or feet
difficulty doing up buttons and picking up small items
loss of feeling especially in the hands and feet
problems with balance or walking, and clumsiness
be safe. If you notice changes in your walking, stance, fine and gross motor skills, or balance speak to your doctor as soon as possible and ask for a referral to an occupational therapist, exercise physiologist or physiotherapist.
Tips to manage peripheral neuropathy | Ngā kupu āwhina mō te whakahaere Pūtau Iotaiaki Mōwaho:
use a night light so that you don’t trip or bang into anything if you need to go to the toilet at night
keep clutter and rugs off the floors
have clear paths to the toilet and bedroom
use handrails where possible
use nonslip mats in the shower and bathroom
be careful on slippery and wet floors
do not walk around bare footed as you may not notice if you stand on something that could damage your feet
wear shoes and slippers that fit well
use a walking stick if you need to
wear gloves when washing up, cleaning and gardening
test water temperature with your elbow
take care when cutting food and opening cans or jars
keep your skin moisturised to prevent cracking
check your hands and feet daily for signs of injury, rubbing, redness or infection
ask for help if you need it, e.g., to do up buttons and shoes
find clothes and shoes that are easy to put on and take off
avoid driving if symptoms are severe.
Alerting your healthcare team of side effects | Whakaohititia tō rōpu tiaki hauora ki ngā mate āpiti
Your health care team wants to hear about your side effects. Your questions and concerns are important. Do not be afraid to share them. Ask your health care team who you should contact if you feel that your side effects need assessing right away.
Treatment changes | Ngā pānonitanga maimoa
Occasionally, if you have severe side effects, your doctor may discuss delaying or changing your treatment to prevent further discomfort.
Start a symptom diary | Tīmatahia he rātaka tohumate
Keeping track of your symptoms can help you and your cancer care team to manage them better.
Know who to contact if you have a problem | Me mōhio hoki ki te whakapā atu ki a wai mēnā he raru tāu
Ask your doctor or nurse:
when you should call for help or advice
who you should contact
how to contact them (including at night or weekends).
Keep this information where you can easily find it.
Our partners at the Pancare Foundation have created a webinar to help patients manage these side effects and help you navigate each day and experience greater quality of life. Pancare's experts share their knowledge surrounding common side effects such as nausea, peripheral neuropathy, fatigue, mouth sores, abdominal discomfort and more. Practical ways to manage these side effects are explored along with information regarding the support and care available for you and your family.
*NB - The PanSupport service mentioned is not available to patients in New Zealand
Diet & Nutrition
Whiringa kai me te taioranga

Why is diet and nutrition important? | He aha e whaitikanga ai te whiringa kai me te taioranga?
You may be feeling that some things are out of your control, however there are a number of actions that you can take to make sure your body is in the best condition to cope with, and heal from, the symptoms and side effects of the cancer and cancer treatments.
Below you will find detail about why diet and nutrition can make a big difference to the healing process and how you feel.
Why does oesophageal cancer affect nutrition? | He aha e pāngia ai te mate pukupuku pūkai i te taioranga
Oesophageal cancer, and cancer treatments place extra demands on your body. They can also cause you to lose your appetite and energy, putting you at an increased risk of malnutrition. It is important to ensure that your body is receiving the right nutrition before, during and after treatment to be able to cope with these extra demands.
Your food choices when you have cancer and are undergoing treatment may be very different from what you are used to eating.
The main goal is to try to keep your weight constant, maintain muscle strength, maintain a healthy weight, and have more energy, all of which help your body to heal properly, improve your quality of life and give you the energy to cope with all the new challenges treatment may bring.
Oesophageal cancer and the treatments for oesophageal cancer may impact | Ka pāngia pea e te mate pukupuku pūkai me ngā maimoatanga e hāngai ana:
your nutritional requirements and what you need to eat
how much you eat
your appetite
your ability to digest food
your ability to maintain your weight and muscle mass
your energy levels and general wellbeing.
Good nutrition can help to | He mea āwhina te taioranga pai ki te:
manage the side effects of treatment
speed up recovery after treatment
heal wounds and rebuild damaged tissues after surgery, radiotherapy, chemotherapy, or other treatment
improve your body’s immune system and ability to fight infections.
Overall, try to make food choices that provide you enough | Nā reira, me ngana ki te whiriwhiri i ngā kai ka whakaratoa ki a koe:
calories (to maintain your weight)
protein (to help rebuild tissues that cancer treatment may harm)
nutrients such as vitamins and minerals
fluids (essential for your body’s functioning).
Exercise can also help with appetite and digestion issues related to treatment.
Nutritional tips during treatment | He kupu āwhina taioranga e koke ai te maimoatanga
Click here to learn more about nutritional tips during treatment | Pāwhirihia ki kōnei mō ētahi atu whakamōhiotanga
To maintain good nutrition | Kia mau roa ki te taioranga pai:
you may need more energy (kilojoules/calories)
eat small, frequent meals or snacks, rather than three large meals a day
ask for a referral to a dietitian – discuss eating issues, weight issues, muscle loss
do some light physical activity, such as walking, to improve appetite and mood, reduce fatigue, help digestion, and prevent constipation
check with your doctor or dietitian before taking vitamin or mineral supplements or making other changes to your diet
relax dietary restrictions, e.g., choose full-cream rather than low-fat milk
consider using nutritional supplements if you cannot eat enough – discuss options with your doctor, palliative care specialist or dietitian.
Nutritional tips following surgery | Ngā kōrero āwhina taioranga whai muri i te pokanga
Click here to learn more about nutritional tips following surgery | Pāwhirihia ki kōnei mō ētahi atu kupu āwhina taioranga
Surgeries used to treat cancer may result in a variety of side effects, including weight loss and diarrhoea. The side effects usually only last for a short period of time, but you may have to make some changes to your diet to ensure that you are getting enough nutrition and maintaining your weight.
Your body needs good nutrition after surgery, and it is an important part of your recovery process. If you are struggling to eat or drink, the hospital may prescribe nutrition supplements, or recommend tube feeding, to help you to maintain weight and provide you with the nutrients you need for speedy recovery.
Tips on maintaining weight after surgery | Ngā kupu āwhina ki te whakataki taumaha whai muri i te pokanga:
monitor your weight – weigh yourself once or twice a week to monitor for any weight loss
if you are losing weight, tell your doctor and get a referral to see a dietitian
eat small, frequent meals after surgery so your digestive system only has to deal with a small amount of food at a time.
We recognise that dietary changes have a huge impact on everyone with cancer. It can take a while to get used to changes to your diet and lifestyle but finding ways to manage your diet and symptoms can help you feel more in control. It can also be helpful to speak to your dietitian, doctor or nurse.
Living well with cancer
Kia ora pai ai

Learn more about living with cancer.
Read about other people’s cancer journeys see our personal journeys page.




Useful Websites & Patient Support | Ngā pae tukutuku whai take me ngā wāhi āwhina tūroro
DISCLAIMER: Information provided by the Gut Cancer Foundation should be discussed with your healthcare professional and is not a substitute for their advice, diagnosis, treatment, or other healthcare services. In some cases, information has been gathered from international sources and should be discussed with New Zealand health care professionals.